Erythema Ab Igne is a skin reaction which occurs in response to repeated exposure to infrared radiation in the form of heat. This could be from the use of heating pads, space heaters and laptops. It presents as a localized fish-net like pattern of hyperpigmentation on the skin. The lesion is usually asymptomatic. The pathophysiology is not well understood, but according to Kettlehut (2022), repeated exposure to the heat damages superficial blood vessels and leads to large deposits of hemosiderin under the skin. Hemosiderin is a protein compound that stores iron in the tissues. Accumulation of hemosiderin under the skin then results in a brown or black staining of the skin (hyperpigmentation). Erythema ab igne usually resolves on its own once the offending heat source is eliminated, but the hyperpigmentation may persist, in which case topical tretinoin, hydroquinone and laser therapy can be used to improve the appearance.

The majority of the cases of erythema ab igne have been reported in middle-aged and elderly adults with musculoskeletal pain who constantly use hot water bottles or heating pads to alleviate their pain. In younger adults, the lesion has been frequently associated with the use of laptops or space heaters (Ly, 2021).
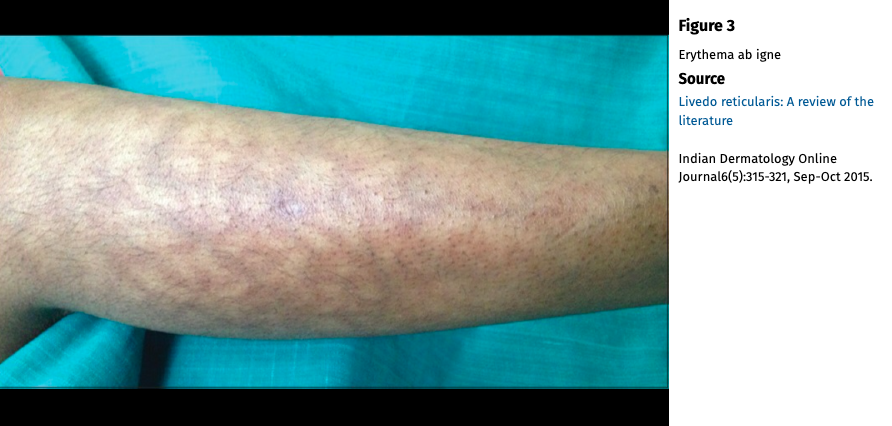
Erythema ab igne can resemble other conditions such as livedo reticularis and livedo racemosa, to name a few. The figures below illustrate the clinical presentation of the three conditions: livedo reticularis, livedo racemosa and erythema ab igne.


In rare cases, malignant transformation to squamous cell carcinoma (SCC) or Merkel cell carcinoma can occur (Ly, 2021; Kettlehut, 2022). Wipf (2022) presents an interesting case report of such a case, which also has some ethical dilemmas involved. The case report is of a 48-year old male with a history of chronic lower back pain, for which he had been using a heating pad, and a 15-year history of a rash on his lower back at the site of heat exposure. Four years ago, a suspicion lesion (later confirmed as well-differentiated SCC) had developed within the rash, but the patient declined treatment because he felt like it had resolved after the biopsy. Now, three years later, another tender lesion had developed near the biopsy site. He was referred to the dermatologist for further management. The dermatologists were concerned about a multifocal SCC. Several biopsies were performed. After the pathology results were received, Mohs surgery was successfully completed. The patient was then counseled on the risk of continuing to use the heating pad and the risk of developing new SCCs, but the patient clearly stated that he would not discontinue using the heating pad despite the risks because he felt like it was the only treatment that helped with his back pain. The case report doesn't include any other information about what was done and what happened to the patient, but this is definitely a difficult situation to be in as a healthcare provider. Our role as a provider is to educate and inform patients of the risks and benefits and help them make informed decisions, but then ultimately, the patient has the final say and whatever decision they make, we may have to respect that. But what if the voluntary decision the patient (fully alert, aware and capable of making his own decisions) makes may harm him in the long term..? What do you do in that case? In the case of this 48 year-old patient, it seems like one of the first things is to make sure that the patient receives proper treatment and management of his back pain. It is also important to ensure that the provider frequently follows-up with the patient so that the patient can be closely monitored for potential recurrence of SCC. To make sure that the patient follows up as recommended, it is necessary that the provider builds trust with the patient and makes sure that the patient feels heard and supported during every visit. The provider may also prescribe topicals, if there are any available, that can help prevent future SCCs. For example, topical 5-fluorouracil is often used to treat precancerous lesions/actinic keratosis and can be prescribed after Mohs’ surgery to prevent development of SCC in the same area (Robins, 2004). The patient should also be encouraged to contact the clinic with any questions or concerns he may have.
References:
Kettlehut A. E., Traylor, J, Roach, P. J. (2022). Erythema Ab Igne. StatPearls.
https://www.ncbi.nlm.nih.gov/books/NBK538250/
Ly, V., Vandruff, E. J., Fashner, J. (2021). Erythema Ab Igne: Toasted Skin Syndrome. HCA Healthcare Journal of Medicine, 2 (2). doi: https://doi.org/10.36518/2689-0216.1149
Robins, P., Hale, E. (2004). Topical 0.5% Fluorouracil Treatment Following Mohs’ Surgery For Squamous Cell Carcinoma For The Prevention Of Future Squamous Cell Carcinoma. Journal of the American Academy of Dermatology, 50 (3). doi: https://doi.org/10.1016/j.jaad.2003.10.035
Sajjan, V., Lunge, S., Swammy, B. P., Pandit, M. A. (2015). Livedo Reticularis: A Review of the Literature. Indian Dermatology Online Journal, 6 (5), 315-321. doi: 10.4103/2229-5178.164493
Wipf, J. A., Brown, R. M. (2022). Malignant Transformation of Erythema Ab Igne. JAAD Case Reports, 26, 85-85. doi: https://doi.org/10.1016/j.jdcr.2022.06.018

No comments:
Post a Comment